Why those tiny black spots keep stealing your focus
You look up from your phone and there it is again: a speck or thread that drifts across your vision, darting away when you try to look directly at it. For many people these annoyances are a daily companion. They are distracting, a little creepy, and sometimes enough to send someone into an internet-fueled spiral of worry. The good news is that most of the time these little visitors are harmless, and the eye has perfectly good reasons for producing them.
Understanding what those spots are, why they appear, and when they signal something serious helps you replace anxiety with agency. You will learn how the eye’s anatomy makes floaters possible, the common triggers, how to tell a harmless floater from an emergency, and what treatments actually work versus the myths that don’t. Think of this as an eye-level adventure: we will go from the clear crystalline center of your eye to the jelly-like gel where the floaters live, then back to practical steps you can take today.
Along the way there will be a couple of small surprises. You will meet named conditions like posterior vitreous detachment, discover how eye movement changes floater behavior, and learn how modern medicine sometimes removes these nuisances and sometimes advises patience. By the end you should feel a lot calmer, a bit smarter, and ready to talk to your eye doctor without panic or confusion.
What those black spots really are, in plain English
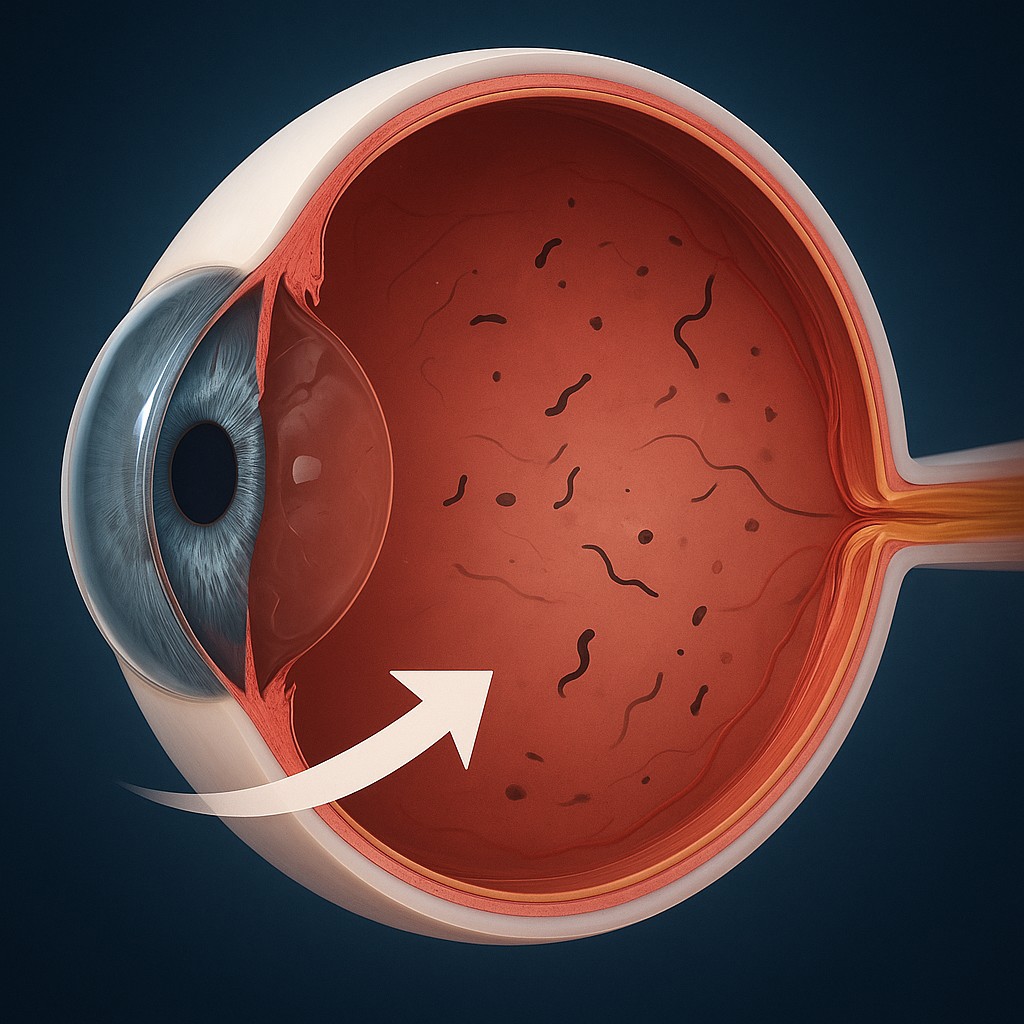
Most of the time the black spots are called floaters. They are tiny bits of cellular debris or clumps in the vitreous, the clear, gel-like substance that fills the middle of the eye. When light enters the eye, these particles cast shadows on the retina, the light-sensing layer at the back of the eye. Your brain interprets those shadows as specks, threads, cobwebs, or squiggles that seem to drift when you move your eyes.
Floaters come in different shapes and sizes. Small round dots are common. Long, stringy lines or cobweb shapes suggest more fibrous material. Sometimes floaters are so faint you only notice them against a bright sky or a white screen. They are more noticeable when you look at a plain, bright background. That movement you see is real - the floater moves when your eye moves - but the object itself is inside your eye, not outside in the air.
There are other phenomena that can look like floaters but are not. For example, the blue-field entoptic phenomenon makes you see tiny bright dots moving rapidly when you look at a clear blue sky. Ocular migraine aura produces shimmering zigzag patterns and temporary blind spots. Visual snow is a constant grainy static across the whole field. Learning the differences helps you and your clinician decide what to do next.
Why floaters appear - the usual suspects and the mechanics
As we age the vitreous gel naturally changes. It slowly liquefies and shrinks, a process called syneresis. When the gel contracts it can clump and pull away from the retina, forming a posterior vitreous detachment, or PVD. A PVD is the most common cause of floaters, and it becomes more likely after the age of 50. PVD itself is often harmless, but because the vitreous can tug on the retina, it can occasionally cause a retinal tear, which is a medical emergency.
Other risk factors make floaters more likely. Nearsighted people tend to develop floaters earlier because their eyes are slightly longer, which stresses the vitreous. Eye trauma or inflammation, prior eye surgery such as cataract extraction, and some retinal diseases can all increase floater risk. Infections or inflammatory conditions can create floaters made of inflammatory cells, while bleeding inside the eye will give you dark spots from blood.
So the mechanics are straightforward: changes in the vitreous produce debris or gaps that cast shadows on your retina. Your brain sees those shadows as moving spots. The degree of bother depends less on how big the floater is and more on its location relative to the visual axis. One small floater sitting right in the center of your visual field can be endlessly irritating while larger floaters at the edge of your vision may go unnoticed.
How to tell a harmless floater from something urgent
Not all sudden floaters are created equal. A slow appearance of a few floaters in older adults that do not come with flashes of light or vision loss is usually benign and can be managed conservatively. However, certain warning signs warrant immediate medical attention:
- A sudden shower or large increase in the number of floaters, particularly if new flashes of light appear, suggests that the vitreous may have pulled on the retina, possibly causing a tear.
- A shadow or curtain creeping across part of your vision indicates a possible retinal detachment, which requires urgent treatment to prevent permanent vision loss.
- Significant loss of vision, severe pain, or redness with floaters are not typical for simple floaters and should be evaluated promptly.
If you experience any of these red-flag symptoms, see an eye specialist without delay. Retinal tears and detachments are time-sensitive; the sooner they are found and treated, the better the chance of preserving vision.
What the doctor will do and what to expect during the exam
When you see an eye doctor for floaters, expect a careful history and a dilated eye exam. The doctor will ask about timing, associated symptoms like flashes or shadows, and any history of trauma or surgery. Pupil dilation is important because it allows the clinician to examine the retina and vitreous more thoroughly using special lenses and lights.
If the view is limited because of dense floaters or bleeding, your eye doctor may use ocular ultrasound to look behind the cloudiness and assess for retinal detachment. Optical coherence tomography, or OCT, is another imaging tool that gives high-resolution cross-sectional images of the retina and can help detect subtle changes.
The critical goal of the exam is to rule out retinal tears or detachment. If everything looks stable and the floaters are from a posterior vitreous detachment, your doctor may simply monitor you and explain the signs that should prompt a return visit.
Treatment options - patience, lasers, and surgery
Most floaters do not need treatment. The brain often adapts, learning to ignore the shadows over weeks to months. Here are the main management paths a doctor might discuss:
- Observation and reassurance. For stable floaters that are not causing major functional problems, the typical advice is to watch and wait. Many people report that floaters fade into the background or become less bothersome with time.
- Laser vitreolysis. This outpatient procedure uses a focused laser to break up or vaporize floaters. It can be helpful for certain kinds of floaters, especially those well away from the retina and lens. Outcomes vary, and the procedure is not suitable for all types of floaters. Risks include retinal injury and incomplete removal.
- Pars plana vitrectomy. This is a surgical removal of the vitreous gel and its debris. Vitrectomy can dramatically reduce floaters but carries risks such as cataract formation, infection, retinal tear or detachment, and increased intraocular pressure. Because of these risks, vitrectomy is usually reserved for cases in which floaters cause severe, ongoing visual disability.
- Pharmacologic vitreolysis. Research is ongoing into drugs that could liquefy or dissolve vitreous opacities. None of these treatments are yet widely established as routine care.
Choosing between these options depends on how much the floaters interfere with daily life, the exact nature and location of the floaters, and the risks you are willing to accept. A frank conversation with a retina specialist helps balance potential benefit versus harm.
Simple, practical ways to live with floaters
If your eye doctor confirms that your floaters are not a threat, several strategies can reduce their nuisance value and help you cope day to day. First, lighting and contrast matter. Floaters are more visible against bright, plain backgrounds like the sky, a computer screen, or white walls. Wearing sunglasses outdoors and using soft ambient lighting instead of glaring overhead lights can help.
Eye movement can momentarily shift floaters out of your direct view. A deliberate look up and down or side to side can reposition the floater, and blinking often helps settle them. Practicing relaxed focus, rather than staring intently at the floater, reduces the attention paid to it and allows the brain to habituate more quickly.
Keep a floater diary if the problem is new or changing. Note when you first saw it, whether it increases or decreases, and any accompanying flashes or vision changes. This record is useful for follow-up visits and helps your doctor decide whether imaging or intervention is warranted.
Clearing up common myths and misunderstandings
People come with plenty of ideas about floaters, and not all of them are grounded in evidence. Here are some common myths and the reality behind them:
- Myth: Floaters are in your brain, not your eye. Reality: Floaters are shadows cast inside the eye by debris in the vitreous. They are ocular, not neurological.
- Myth: Eye drops or supplements will dissolve all floaters. Reality: No eye drop has been proven to reliably eliminate floaters. Some supplements support eye health, but they will not remove established vitreous clumps.
- Myth: Floaters always mean you will go blind. Reality: Most floaters are benign and do not threaten sight. Only when they signal retinal tearing or detachment does urgent intervention become necessary.
- Myth: You can train your eyes to stop seeing floaters instantly. Reality: While the brain can habituate over time, there is no guaranteed short-cut to instant disappearance apart from invasive removal.
Dispelling these myths reduces unnecessary fear and helps you approach the issue with realistic expectations.
Quick comparisons: floaters and other similar visual experiences
| Phenomenon |
Typical appearance |
When it happens |
Usual management |
| Vitreous floaters |
Round dots, threads, cobwebs that drift |
More visible against bright backgrounds; often with age or after PVD |
Observation, possible laser vitreolysis, or vitrectomy for severe cases |
| Ocular migraine aura |
Shimmering zigzags, flickering lights, temporary blind spots |
Often lasts 10-30 minutes, may precede headache or occur alone |
Reassurance, neurology or eye evaluation if atypical |
| Visual snow |
Constant grainy static across vision |
Persistent and diffuse, not localized |
Neurology referral; management is challenging |
| Blue-field entoptic phenomenon |
Tiny bright dots moving rapidly |
When looking at clear blue sky |
Benign and normal |
| Retinal detachment symptoms |
Sudden increase in floaters, bright flashes, shadow or curtain |
Often acute and progressive |
Urgent retinal surgery required |
This table highlights how similar-looking visual symptoms have very different causes and consequences. Matching features to cause helps prioritize action.
How to talk to your doctor - questions that get useful answers
When you see an eye specialist, being prepared makes the visit more productive. Useful questions include: Is there any sign of retinal tear or detachment? Do my floaters suggest a posterior vitreous detachment? Are there non-surgical options that might help in my case? What are the likely benefits and risks of laser vitreolysis or vitrectomy for my situation? How should I monitor my vision and when should I return?
Bring your floater diary, a list of symptoms, and any relevant medical history like prior eye surgery. If you have sudden changes in vision, ask for a prompt dilated exam; waiting can be risky in some cases.
A final note to keep you curious and calm
Floaters are a fascinating intersection of anatomy, physics, and perception. Tiny particles in a transparent gel casting shadows on a living retina produce a subjective experience that can be oddly captivating and frustrating at once. The encouraging part is that most floaters are not dangerous, and your eye has mechanisms and many specialists who know how to manage them.
If your floaters are new, changing rapidly, or accompanied by flashes or a loss of vision, act quickly and seek an eye exam. If they are stable and manageable, give your brain a few weeks to learn to ignore them, try simple coping strategies, and keep your eye health routine up to date. Either way, you are now better equipped to understand what those black spots are, weigh your options, and talk to your doctor with confidence. Consider this your small victory in ocular literacy - when your next floater appears, you will know its story and how to respond.